

Enclosure (3) to COMDINST 1750.4D
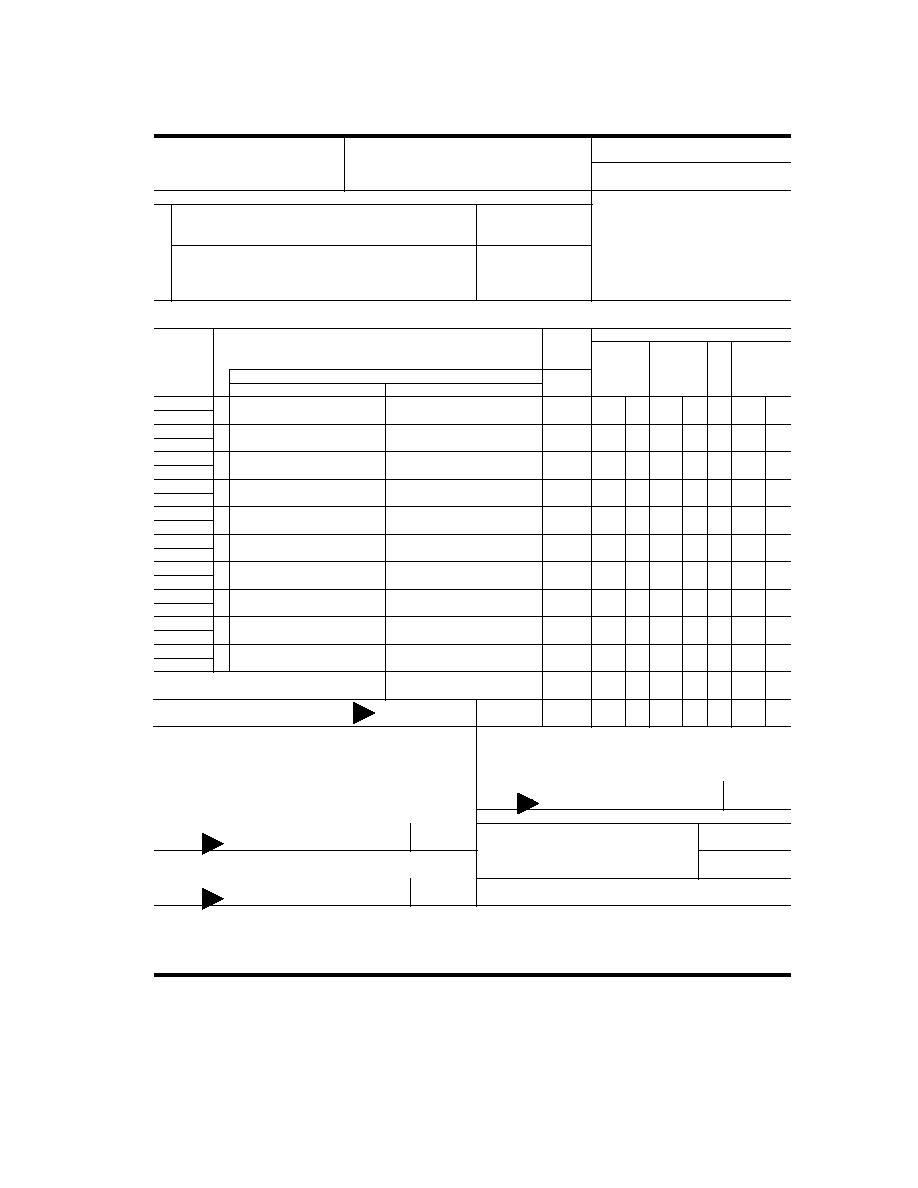
1. DEPARTMENTOR ESTABLISHMENT, BUREAU, DIVISION OR OFFICE
2. VOUCHER NUMBER
CLAIM FOR REIMBURSEMENT
FOR EXPENDITURES
3. SCHEDU LE NUMBER
ON OFFICIAL BUSINESS
5. PAID BY
Read the Privacy Act Statement on the back of this form.
a. NAME (Last, first, m iddle i nitial)
b. SOCIAL SECURITY NO.
4.
d. OFFICE TELEPHON E NUMBER
c. MAILING ADDRESS (Include ZIP Code)
6. EXPENDITURES (If fare claimed in col. (g) exceeds charge for one person, show in col. (h) the number of additional persons which accompanied
the claimant.)
DATE
Show appropriate code in col. (b):
MILEAGE
C
AMOUNT CLAIMED
RATE
A - Local travel
O
B - Telephone or telegraph, or
D
ADD.
TIPS AND
19
FARE
E
C - Other Expenses (itemized)
MILEAGE
PER-
MISCEL-
OR TOLL
SONS
LANEOUS
NO. OF
(Explain expenditures in specific detail.)
MILES
(a)
(b)
(c) FROM
(d) TO
(e)
(f)
(g)
(h)
(i)
SUBTOTALS CARRIED FORWARD FROM THE
If additional space is required continue on the back.
BACK
TOTALS
$
7. AMOUNT CLAIMED (Total of cols (f), (g) and (i).)
8. This claim is approved. Long distance telephone calls, if shown, are certified as
10. I certify that this claim is true and correct to the best of my knowledge and
belief and that payment or credit has not been received by me.
necessary in the interest of the Government. (Note: If long distance calls are
included, the approving official must have been authorized, in writing, by the head of
the department or agency to so certify (31 U.S.C. 680a).)
Sign Original Only
Sign Original Only
DATE
CLAIMANT
SIGN HERE
11.
CASH PAYMENT RECEIPT
DATE
a. PAYEE (Signature)
b. DATE RECEIVED
APPROVING
OFFICIAL
SIGN HERE
9. This claim is certified correct and proper for payment.
c. AMOUNT
$
Sign Original Only
DATE
12. PAYMENT MADE
AUTHORIZED
CERTIFYING OFFICER
BY CHECK NO.
SIGN HERE
ACCOUNTING CLASSIFICATION
STANDARD FORM 1164 (Rev. 11-77)
Prescribed by GSA, FPMR (CFR 41) 101-7

 Previous Page
Previous Page
